What is Cubital Tunnel Syndrome?
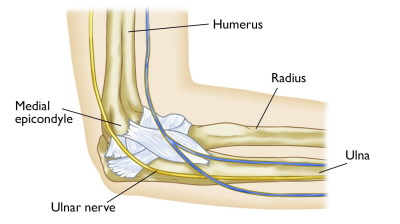
The ulnar nerve runs from the neck, down the arm, and around the inside of the elbow (the ‘funny bone’).
At the elbow it passes through a narrow tunnel of bone and tissue called the cubital tunnel.
If the nerve becomes compressed here, it can cause:
• Numbness/tingling in the ring and little fingers
• Weakness of grip and fine finger control
• Pain around the elbow or forearm
• Wasting of hand muscles if severe or long-standing.
Why might I need surgery?
Surgery is considered if:
• Symptoms persist or worsen despite splints, rest, and activity modification
• Weakness or muscle wasting develops
• Pain or tingling interferes with work or daily activities
The goal is to relieve pressure on the ulnar nerve and prevent long-term damage.
What does the operation involve
The operation is called Cubital Tunnel Release
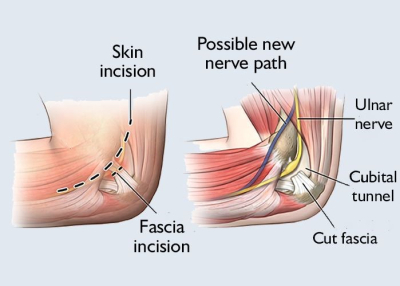
• A cut is made on the inside of the elbow.
• Structures compressing the nerve are released.
• Sometimes, the nerve is moved to a new position in front of the elbow (anterior transposition).
• In some cases, part of the bone (medial epicondyle) is removed to create more space (medial epicondylectomy)
The choice of technique depends on the severity of compression, elbow anatomy, and surgeon preference. The procedure usually lasts 30–60 minutes and most patients go home the same day.
Pre-operative Assessment
Before your surgery, a member of the pre-operative team will contact you to discuss your health and medical history. They may ask about any medications you are taking, allergies, and other relevant health conditions. This helps the surgical team plan your care and ensure you are fit for the procedure. You may be asked to attend a pre-assessment appointment if necessary.
Fasting Instructions
Before Sedation It is very important to follow fasting instructions before your procedure:
• Do not eat any food for 6 hours before the procedure.
• You may drink clear fluids (such as water, black tea, or black coffee without milk) up to 2 hours before the procedure.
• Do not eat or drink anything within 2 hours of the procedure.
What are the risks?
As with all surgery, risks exist though serious complications are uncommon:
• Infection or bleeding
• Stiffness and soreness around the elbow
• Scar tenderness
• Nerve injury (rare, but may worsen symptoms)
• Incomplete recovery, especially if nerve compression was long-standing.
Specific risks of cubital tunnel surgery
• Nerve problems
The ulnar nerve or nearby small nerves can be irritated or injured. This may cause numbness, tingling, or soreness around the elbow or forearm.
Rarely, nerve damage can cause lasting weakness or loss of feeling in the hand.
• Persistent or recurring symptoms
Sometimes numbness, tingling, or weakness do not completely go away, especially if the nerve was badly compressed before surgery.
In some cases, symptoms can return months or years later.
• Nerve instability
The ulnar nerve may move out of place (sublux) when the elbow bends, which can cause snapping or discomfort.
• Elbow stiffness or reduced movement, usually temporary.
• Complex regional pain syndrome (CRPS) – a rare condition that causes prolonged pain and swelling after surgery.
• Additional risks if the nerve is moved (anterior transposition)
More bruising, swelling, or scarring because of extra dissection.
A small risk of damage to another skin nerve, which can leave a patch of numbness on the inner forearm.
The moved nerve may not stay in its new position, which can cause ongoing irritation.
👉 Most people notice improvement in tingling or weakness within weeks to months, though recovery can be slower if the nerve was badly affected before surgery.
After Surgery – Rehabilitation
First 1–2 weeks
It is important to continue your usual pain medications until you feel the benefit of the injection. Do not stop strong painkillers (such as morphine, gabapentin, pregabalin or amitriptyline) suddenly – your GP or consultant will advise you on tapering them if necessary.
• Arm in a light dressing
• Move fingers, wrist, and shoulder immediately
• Begin elbow bending/straightening within days
• Stitches removed at 10–14 days
Weeks 2–6
• Gentle elbow stretches
• Nerve gliding exercises with physiotherapy
• Light hand use (writing, typing, light household tasks)
• Driving possible after ~2 weeks if comfortable (avoid driving while your arm is in a bulky dressing or sling). You must have enough control of the steering wheel, gears and indicators before attempting to drive.
Weeks 6–12
• Strengthening hand and forearm exercises
• Gradual return to work and sport (manual work may take 8–12 weeks)
Recovery time varies; long-standing nerve compression may mean numbness/weakness takes months to improve or may not fully recover.
Exercise Program (guided by your physiotherapist)
• Finger mobility: make a fist, spread fingers, repeat 10x several times daily
• Elbow bends: bend and straighten gently
• Nerve glides: extend arm to the side with palm up, gently tilt head away; repeat 5–10x
• Strengthening: squeeze a soft ball, light wrist curls, resistance band exercises (after 6 weeks).
Follow-up
A follow-up will be arranged by Mr Al-Mahfoudh’s PA, for a clinic appointment to check the wound and recovery progress.
If you develop:
• Severe pain, swelling, or bleeding
• Fever, redness, or discharge from the wound
• Sudden loss of movement or sensation
Contact your surgical team or GP immediately.
For further information / contact us
Mr Al-Mahfoudh’s PA
07501 703075
secretary@spineandbrain.co.uk
Pre-operative team at Spire Gatwick
01293 306 122
gphpre-assessment@spirehealthcare.com
Pre-operative team at Spire Montefiore
01273 829 350
montefioreadmissionspsc@spirehealthcare.com